Reliable information about MDMA is hard to come by in the United States. Despite the fact that about 19 million Americans had used MDMA as of 2017,1 most people don't seem to know much about MDMA, even users of the drug. Proper drug education is absent from American schools and I'm angry about it. Hopefully writing this will make me a little less angry. In this post I'll give what I think is an accurate and evidence-based perspective on MDMA, including its history, its long-term risks and non-risks, and the properties that make it a beautiful work of chemical art (yeah, I said it). I’m hoping three things for people who read this post: that you’ll at least be sympathetic to my description of MDMA as penicillin for the soul, that you’ll be much less likely to get hurt if you decide to try MDMA, and that you’ll consider donating to MAPS (Multidisciplinary Association for Psychedelic Studies), because they could really use some more funding. A fourth and smaller hope is that you’ll become a fan of Alexander Shulgin, because he was amazing and is underappreciated.
I should acknowledge that this post will be full of opinions and judgements, so it’s definitely not objective. Also, I’m not a scientist, so my thoughts about studies probably shouldn’t be trusted. I think my perspective is worth reading anyway. It includes a lot of sadly uncommon information that everyone should account for, because really, the potential of MDMA applies to everyone. With that in mind, let's dive in!
TABLE OF CONTENTS
What Is MDMA?
The MDMA Experience and After-Effects
The History of MDMA
The MDMA Experience and After-Effects
The History of MDMA
- The Good Part
- The Bad Part
- Make Sure You Buy Pure MDMA
- Don’t Get Arrested
- Know Your Dose
- Stay Hydrated, but Not Too Hydrated
- Try Not To Be on Anything Else, Especially MAOIs
- Don’t Do It If You Have These Health Conditions
- Don't Drive, Even Though You Can
- Wait 3 Months Before Doing it Again
- Conclusion
- Addiction
- Cognitive Deficits
- Depression
- Heart Problems
Bibliography
What Is MDMA?
MDMA is a name for an organic molecule, also known as 3,4-methelenedioxymethamphetamine, as well as the psychoactive compound formed by this molecule, which is what I usually mean when I say MDMA. “Psychoactive” means that MDMA can alter your soul. Like any psychoactive drug, MDMA can cross the partition between your circulatory system and the fluid in your brain, also known as the blood-brain barrier, and manipulate neurotransmitters once it’s in your brain. I think this is incredible! MDMA is also known as ecstasy, X, E, and molly. Yes, the “MA” in “MDMA” stands for “methamphetamine.” No, that doesn’t say anything about its effects. Glad we got that out of the way.
MDMA can be described as a stimulant, an empathogen, and a substituted phenethylamine. It's a substituted phenethylamine because it can be made by switching out (substituting) hydrogen atoms in the chemical structure of phenethylamine, a stimulant produced by the human body. “Stimulant” seems to be kind of a vague term, but it means that MDMA makes you more energetic and alert. The most interesting term here is “empathogen:” this means that MDMA produces feelings of love, emotional connection, and emotional openness. These properties make MDMA a very interesting chemical.
MDMA and penicillin have some interesting similarities. Both are compounds investigated by scientists named Alexander, both are quite safe and consistent in their uses (in fact, MDMA could be significantly safer than penicillin), and in the future we might say that they both revolutionized the treatment of a particular kind of illness. Penicillin is a definitive treatment for bacterial infections. MDMA, with the guidance of a psychotherapist, could be a definitive treatment for emotional trauma and conflict: sicknesses of the soul.
The MDMA Experience and After-Effects
Believe it or not, I’ve never used MDMA, so I can’t tell you what it’s like. What I can tell you is what some scientists have observed about the MDMA experience.Unlike psychedelics like LSD and psilocybin, which produce very complex experiences, MDMA is a pretty simple drug with predictable effects. MDMA is comparable to opiates in its ability to induce a mental state that is “usually pleasurable to almost every user, almost every time.”2 From the review I just cited, MDMA “has been demonstrated to consistently increase levels of understanding, closeness and empathy (Liester et al., 1992; Cami et al., 2000; Sumnall et al., 2006), to encourage an increased thoughtfulness and contemplativeness (Vollenweider et al., 1998a) and to aid a greater exploration of otherwise painful repressed memories, by ‘inhibiting the subjective fear response to an emotional threat’ (Greer and Tolbert, 1986).” This review was written by Ben Sessa and David Nutt, both advocates of MDMA-assisted psychotherapy. They are definitely biased, but they are well-known and reputable scientists (look ‘em up), and Ben Sessa conducts studies on MDMA-assisted psychotherapy, so he has far more personal experience than most researchers.
As of 2015, there were over 80 published laboratory studies on the effects of MDMA on healthy adults, with no drug-related serious adverse effects known to the writers of this review.3 Participants consistently reported feeling loving, talkative, extroverted, sociable, self-confident, friendly, playful, trusting, close to other people, and emotionally concerned.
You might wonder, “Wouldn’t increased trust make it easier for bad people to take advantage of you?” Recent research suggests otherwise. In a study published in January of 2019, researchers at King’s College London asked people on MDMA to play a version of a game called the Prisoner’s Dilemma with both trustworthy and untrustworthy opponents. MDMA increased cooperative behavior when playing trustworthy opponents, but not untrustworthy opponents. The researchers’ explanation is that MDMA increases activity in regions of the brain that are important in understanding the thoughts, beliefs, and intentions of others.4 So there’s that.
There’s a dark side of the MDMA experience. Most recreational users of MDMA believe that they will experience a “hangover” lasting up to a week because of MDMA’s depletion of serotonin in the brain. Users take all sorts of serotonin-raising supplements to cure this “hangover.” A google search of “MDMA hangover reddit” can give you an idea of how much people freak out about this. The MDMA hangover has shown up in studies of recreational MDMA users, but not in clinical research. In its 2016 annual report to the FDA on research of MDMA for treatment of PTSD, MAPS claims that in the week following treatment, “anxiety, fatigue, headache, nausea, needing more sleep, increased irritability, difficulty concentrating, ruminations, and low mood were reported at comparable rates across MDMA and placebo groups.”5 This means that participants felt the same “hangover” whether they took MDMA or an inactive pill. I have a feeling this says something about the role of placebo (or nocebo) in recreational drug use. Recreational drug users in the United States believe, consciously or subconsciously, that drugs are dangerous and bad. This means they experience a range of bad effects that may or may not be caused by the drugs themselves. That’s my guess, at least.
Anyway, here’s the shortest description of the MDMA experience I can come up with: “love.” Love is what MDMA does.
The History of MDMA
The Good Part
MDMA was originally synthesized at Merck in 1912 as a treatment for abnormal bleeding, but it failed to attract much attention in the following decades.6 The story of MDMA as we know it begins more that 50 years later with a chemist by the name of Alexander Shulgin. Much of what I know about the history of MDMA comes straight from the source, PiHKAL (Phenethylamines I Have Known and Loved), specifically Chapter 12, which is about MDMA. In 1965, while experimenting with phenethylamines at Dole Chemical Company, Alexander Shulgin develops a new and easier synthesis for MDMA. He tries it (typical Shulgin). He notes in retrospect that “It was not a psychedelic in itself, but the lightness and warmth of a psychedelic was present and quite remarkable.” He begins testing it on both himself and other willing human subjects.
Shulgin has some fascinating stories to tell about early MDMA experiences. He writes of a student of his at UC Berkeley named Klaus, who takes MDMA, overcomes his debilitating speech impediment, and goes on to start a career in speech therapy. Another one of his subjects, named Janice, takes MDMA and spontaneously asks Shulgin, “Is it all right to be alive?” With Shulgin’s encouragement, she works through her guilt that her mother died in childbirth. Another one of Shulgin’s friends takes MDMA and, within a few hours of open and honest discussion, resolves his emotional trauma following a difficult experience with LSD.
The most amazing result of Shulgin’s experimentation with MDMA is its effect on a psychotherapist friend of his, Leo Zeff (Shulgin calls him Adam in PiHKAL, as this was Zeff’s name for MDMA). At some point in 1977, Zeff is 65 years old and preparing for retirement. Shulgin drops by to introduce Zeff to MDMA. A few days later, Zeff calls Shulgin to say that he’s abandoned his plans for a quiet retirement. He spends the last ten years of his life introducing MDMA to other therapists and teaching them how to use it in practice. At Zeff’s funeral, his wife tells Shulgin that she estimates Zeff ultimately introduced MDMA to some four thousand psychotherapists.
Shulgin ends the chapter with a quote from an unnamed psychiatrist: “MDMA is penicillin for the soul, and you don’t give up on penicillin, once you’ve seen what it can do.”
Later in the book, Shulgin’s future wife describes the aftermath of Shulgin’s decision to temporarily break off relations with her. She is absolutely infuriated, and plans to write a series of letters to Shulgin explaining why she hates him and his other love interest. In a flash of foresight, she decides to take a dose of MDMA first. Her fury gradually dissipates. Half an hour later she decides to call Shulgin to tell him that she loves him and wishes him the best. Tell me this drug doesn’t have the power to save relationships.
Personally, I think Shulgin deserved some kind of award, if not a Nobel Prize, for his resynthesis and investigation of MDMA alone. But, get this: he personally discovered, synthesized, and tested (on himself!) some 230 other psychoactive compounds, in what was effectively a garden shed, with no assistance from authorities aside from a DEA license to research Schedule 1 drugs. Shulgin produced a huge body of knowledge that may never have been developed if he hadn’t taken the personal initiative to investigate. Shulgin risked his own physical and psychological health to realize the potential he saw in these drugs. Isn’t that incredible? And isn’t it unfair that Shulgin died (at the surprisingly old age of 88) with barely a hint of mainstream recognition to his name?
The Bad Part
Here we reach material that Shulgin, understandably, didn’t feel like mentioning in his book. The thing about MDMA is that it’s very enjoyable to use. In fact, Shulgin himself called it his “low-calorie martini.” This means people will pay money for MDMA, and, if they know about MDMA, seek it out just to pay money for it. You can probably guess what this meant for the future of MDMA.
Through the 1970s, the psychotherapeutic community handled the distribution of MDMA with caution. Distributors interviewed by Jerome Beck for The Pursuit of Ecstacy were typically wary of legislation and saw their work as a service to society. The therapeutic mindset of distributors led to a situation of high demand and low supply in the early 1980s, practically begging for some businessman to pick up the slack. Enter Michael Clegg, a former Catholic priest, who took it upon himself to realize the full money-making potential of MDMA. Now, Clegg was not the most scrupulous person ever. Here he is describing how he coined a well-known name for the drug: “I had to convince people who didn’t do drugs to try one no one had heard of. I was telling people it would let them see God. Then it came to me: It was pure ecstasy.”7
I’m not happy about it, but Clegg made his quick buck. His mass-production of MDMA led to a proposal from the DEA to ban it, which led to a backlash from the psychotherapeutic community and extensive media coverage, all of which basically advertised his drug for him. In 1985, Clegg’s production of MDMA grew to some 8,000 tablets per day.8 Yes, Clegg had his fun, and he continued to have fun producing MDMA until he was finally arrested and sentenced to 4 years in prison in 1992. After prison, he changed his name to Satyam Nadeen and became a “spiritual teacher.” Good for you, Michael Clegg.
I wouldn’t mind Clegg’s actions if not for the looming threat of the DEA to safe use of MDMA, which Clegg ignored in favor of fat stacks. On May 31, 1985, the (stupidly overpowered) DEA announced an emergency classification of MDMA. WIth no input required from other government agencies, the DEA placed MDMA in Schedule 1 of the Controlled Substances Act, designating that it had no currently accepted medical use and making it very hard to research--at least, research without the intention of confirming its negative effects. “Isn’t research how we establish a medical use in the first place?” you might ask. Yes, it is.
Let me rephrase this situation. According to the DEA, this chemical that inspired a psychotherapist on the verge of retirement to dedicate the rest of his life to spreading the seeds of MDMA-assisted psychotherapy, building a community of thousands of psychotherapists who use MDMA in their practice, has no currently accepted medical use and does not even deserve investigation into its potential medical uses. Unfair, isn’t it?
Maybe I need to drill a little bit further. Let’s ignore the fact that MDMA has incredible potential for therapeutic use. It’s just a substance. Faced with the spread of an unregulated substance with both potential risks and benefits, the American government does… what? Attempt to regulate the sale of the substance? No. Research the substance honestly? No. Make use and sale of the substance illegal, sending innocent users and vendors of the substance to prison and fueling the growth of an unregulated black market that only exacerbates the risks of the substance? Yeah, for some reason. Tell me, do these seem like the actions of a benevolent authority? In this case, I’m going to say to the American government what it seems to be saying to a large and innocent subset of the American people by its actions: fuck you.*
*I decided to sacrifice nuance here to make a point. I shouldn't blame the whole government. From knowledge that goes as deep as the Wikipedia article on MDMA, it seems like it was mainly Nancy Reagan, a couple senators, and a few people in the DEA, who probably didn’t have malicious intentions themselves--they may have just been deluded by indoctrination and following the rules, which were established earlier by powerful people who definitely had malicious intentions. Anyway, saying “fuck you” to the government is less of a declaration of hostility and more of a motivator for peaceful protest and reform, which I hope any government employee that reads this will take to heart.
How to Obtain and Use MDMA as Safely as Possible, Despite the Best Efforts of the DEA to Hurt You and Make You Hurt Yourself
So, you’re going to a music festival or a rave. You want to try out this exciting drug called MDMA and have a fun and harmless time. Not so fast! There are some things you may want to know before you jump in. I'll assume that you're an adult, whatever that means to you.
I'm including this section not to advocate breaking the law, but to provide valuable information about the risks involved with buying and using MDMA. A lot of people who use MDMA don’t seem to know about these risks.
1. Make Sure You Buy Pure MDMA
Drug testing should be common sense by now. Maybe it would be if drug safety organizations were allowed to operate at music festivals, but in many cases they’re not, so here we are. Let’s say some guy sells you something that he calls MDMA or ecstasy or molly. Is it really MDMA? Potentially not, at least purely, and the guy probably doesn’t know this himself, if he’s not an undercover police officer (unlikely, but they exist). EcstasyData.org, a laboratory pill testing program run by Erowid Center, says that of the samples analyzed in 2019 that were sold as ecstasy, 7% contained MDMA and another drug and 8.8% contained no MDMA, while the rest contained MDMA only. These percentages vary somewhat year to year but have gotten a lot better since the 2000s, when less than a third of samples typically contained MDMA only. Of the samples containing substances other than MDMA, most contained stimulants such as caffeine, amphetamine, methamphetamine, and cocaine, or the MDMA-like drug MDA (which has actually been around for quite a bit longer than MDMA). Several contained 2C-B, also a very interesting drug and Alexander Shulgin’s favorite psychedelic. A few contained drugs with cool names like methylsulfonylmethane, N-ethylpentylone, and 5-MeO-DiPT, which I would not mind getting instead of MDMA.9
Point is, the only way to know for sure is to use an MDMA test kit. Testing involves putting a drop of dye on your drug and hoping it will turn a certain color. You can find good test kits by looking up “bunk police mdma test kit” or “dancesafe mdma test kit.” Before buying what might be MDMA, test it. If it doesn’t test as MDMA, politely decline. You’re doing a favor to both yourself and the person who’s offering to sell it to you.
The problem with MDMA test kits is that they only test for the presence of MDMA, not its purity. For all you know, your MDMA could still be laced with whatever. To be more confident, you can also test for fentanyl, fentanyl analogs, and methamphetamine (to read how, follow the footnote).10 Again, if drug safety organizations could operate at music festivals, they could test the quality of your MDMA, but oftentimes they are not allowed to do this. This is stupid. Even more stupid than the fact that MDMA is illegal, which is why this problem exists in the first place.
I feel like I shouldn’t end this part on such a depressing note. A safer way of obtaining MDMA than getting it from a stranger at a festival is to have it delivered to you through the darknet. Darknet markets are a marvel of internet communication and a safe and reliable source of drugs of all kinds, as long as you know what you’re doing. There are guides available on Reddit. It should be said that even MDMA obtained from large, well-reviewed suppliers on the darknet is not guaranteed to be pure, so test kits are still worth having.
2. Don’t Get Arrested
The DEA may suck, but it’s also very powerful. Don’t get arrested, unless you plan on using your arrest as an act of peaceful protest, in which case I can’t stop you. Here are some simple ways to lower the risk of being arrested: get MDMA from someone you trust, or the darknet, if you’re confident that you’re using it well; hide your MDMA; bring only as much MDMA with you as you think you’re going to consume; don’t try to bring MDMA on an airplane. If you’re worried about being arrested, feel free to investigate this subject further. Also, if you do get arrested, here’s what you should say to the police: “I won’t answer questions until I have a lawyer.” Anything you say can be used against you in court.
3. Know Your Dose
The experience you get from MDMA depends largely on the dose. Do you know how much MDMA is in that tablet you have? No? Then you might not want to try it.If you really want to do MDMA safely, invest in a milligram scale and buy it in crystallized or powdered form. For a recreational experience, most people use 60-150mg of MDMA, but some people are considerably more sensitive to MDMA than others (yes, that might include you!). Always start low: a light dose is 40-75mg, and common doses for small or sensitive people are in the range of 60-90mg. If you take a dose that’s too high, you’ll experience adverse effects, like vomiting, headaches, and dizziness.11
Luckily, MDMA-related deaths (“overdose” isn’t accurate since these deaths are almost never caused by an excessively high dose) are very rare. The National Programme on Substance Abuse Deaths in the UK estimated in 2006 that 50 MDMA-related deaths occurred in the UK per year in the previous 10 years, 10 of which were attributed solely to MDMA.12 The 2017-2018 Crime Survey of England and Wales estimated that there were 550,000 users of MDMA in the previous 12 months.13 I think the fact that MDMA has gotten more popular in the UK since 2006 can be balanced with the fact that Scotland is not included in the aforementioned survey. I’m going to estimate that, excluding incidents involving multiple drugs, which introduce a plethora of new risks, MDMA contributes to the deaths of 1/50,000 users of MDMA in a given year, assuming that users of MDMA in the UK are representative of all users of MDMA. I don’t know if that was valid statistics but it seems intuitively valid. This statistic seems very low given that the sale and use of MDMA is completely unregulated, which makes it very risky. Most of the deaths attributed to MDMA are due to heatstroke, which I’ll cover in the next section.
4. Stay Hydrated, but Not Too Hydrated
This advice mainly applies to people who plan to dance vigorously, for a long time, in a hot place, because in combination with the rise in body temperature and reduction in body temperature regulation caused by MDMA, this activity can lead to heatstroke. It’s important to note that while MDMA increases risk of heatstroke, heatstroke can happen in these situations even without drug use. For precautions, you can look to DanceSafe, a non-profit and one of the festival drug safety organizations I mentioned earlier. DanceSafe recommends drinking one 1000-2000ml bottle of water, preferably electrolytic, per hour, eating salty snacks, taking breaks from dancing, and staying cool and out of the sun as much as possible. You should eat salty snacks and avoid drinking more than the recommended amount because MDMA inhibits proper intake of water, potentially leading to hyponatremia, a condition caused by an imbalance of water and sodium in the blood.14 Heatstroke is by far the leading cause of MDMA-related hospitalization when no other drugs are involved, although hyponatremia has led to a number of deaths.15
5. Try Not To Be on Anything Else, Especially MAOIs
In general, combining drugs is a bad idea. I have no evidence for this, but after spending a lot of time on online drug forums, I can say that it usually invites unintended consequences. I especially hope you listen to this advice if you’re using antidepressants called MAOIs, which stands for MonoAmine Oxidase Inhibitor. Taking MDMA while using MAOIs can cause serotonin syndrome, a range of symptoms thought to be caused by excess serotonin in the brain, and you definitely don’t want to go there. Serotonin syndrome is potentially fatal and can involve seizures, hypertensive crisis, and extensive muscle breakdown, according to Wikipedia. Contrary to popular belief, SSRIs are not known to interact dangerously with MDMA. In fact, the two drugs seem to reduce each other’s effects, and SSRIs have been proposed to decrease the neurotoxic effects of MDMA.16Also don’t take MDMA with ritonivar, dextromethorphan (DXM), or codeine, as these drugs are all metabolized by the CYP2D6 enzyme and thus can amplify each other’s effects.17
Anyway, if you really want to use MDMA along with another drug, refer to TripSit’s fabulous guide to drug combinations: https://wiki.tripsit.me/images/3/3a/Combo_2.png
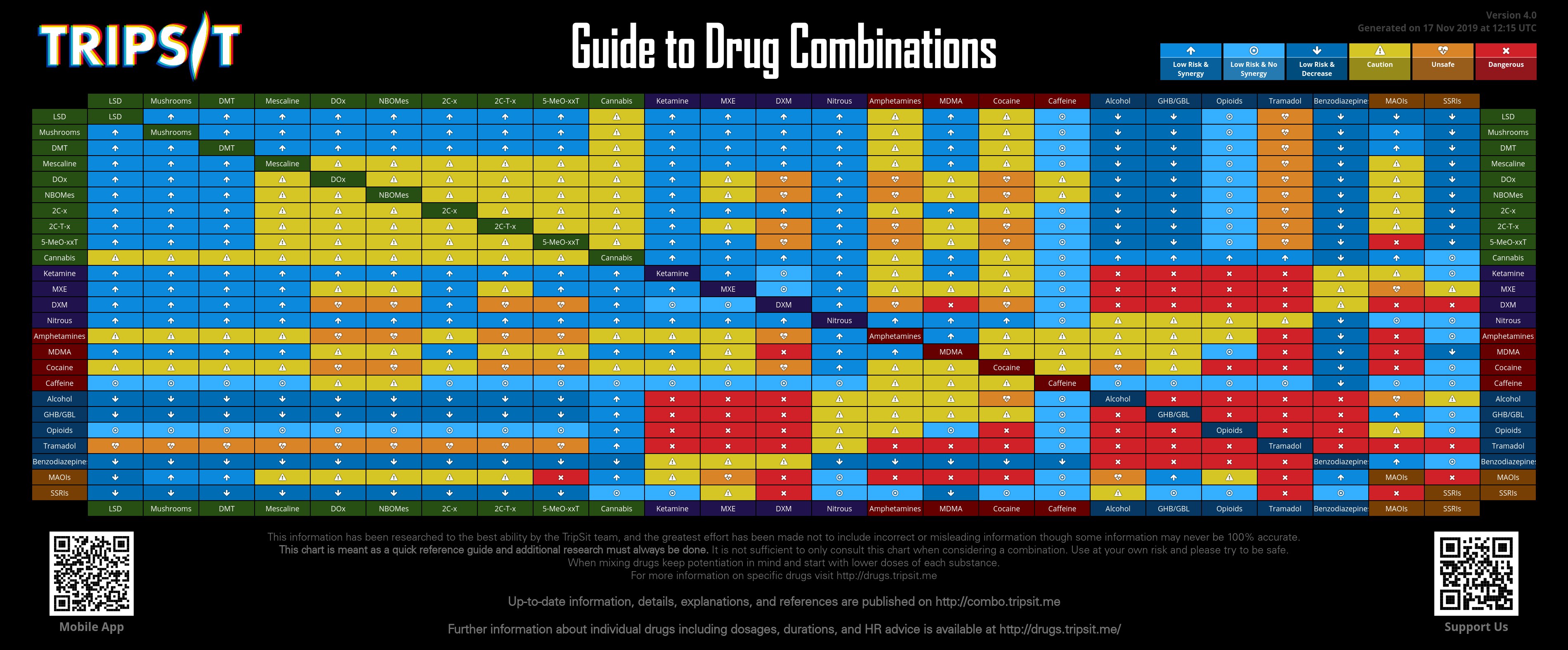{kind=link}
6. Don’t Do It if You Have These Health Conditions
Don’t do MDMA if you’re pregnant. This is common sense. Don’t do MDMA if you have heart problems. According to DanceSafe, MDMA use “causes a modest increase in heart rate and blood pressure, similar to light exercise. While this is not dangerous for a healthy person, it can be quite dangerous for someone with high blood pressure or heart disease.” Any dose of MDMA can cause death in someone with an enlarged heart.18
Don’t do MDMA if you have liver problems, seizures, malignant hyperthermia, or other susceptibility to heatstroke.19
If you have malignant hyperthermia, you may be unaware of it. Malignant hyperthermia is a rare genetic condition. If your parents have it or you have any first or second degree relatives who have experienced bad reactions to general anaesthesia, specifically a rise in body temperature and severe muscle contractions, you could have it.20
7. Don't Drive, Even Though You Can
If a police officer could tell that you're not sober, you shouldn't drive, or you risk getting a DUI. It's probably best never to risk it. You should have a designated driver, and otherwise there's always Uber or taxis.
“In the hours after taking the drug, MDMA produces significant reductions in perceiving and predicting motion—for example, the ability to judge whether a driver is in danger of colliding with another car. This emphasizes the potential dangers of performing complex or skilled activities, such as driving a car, while under the influence of this drug.”
This is the only information given about MDMA and driving. The footnote at the end of this paragraph links to one study on the effect of MDMA on psychomotor skills and attention. The abstract of this study says that 75mg MDMA was found to improve psychomotor performance and impair ability to predict object motion under divided attention. MDMA had no effect on visual search, planning, and retrieval from semantic memory.1 This is a mixed bag and tells us nothing about MDMA and driving, yeah?
A review of the actual effects of up to 100mg MDMA on driving performance concludes that MDMA improves some psychomotor driving skills when administered during the day, and does not affect driving performance overall. Also, people who were sleep deprived and on MDMA drove as poorly as people who were sleep deprived and not on MDMA. The writers think that this is relevant somehow because people stay up all night “raving” when they do MDMA (yes, they use quotes). Their conclusion is that “MDMA cannot compensate for the impairing effects of sleep loss and drivers who are under the influence of MDMA and sleep deprived are unfit to drive.”22 What?????
Clearly, the lesson here is that you should avoid driving while sleep deprived.
8. Wait 3 Months Before Doing It Again
There are certain risks that may come with regular use of MDMA, which I’ll cover in the next section, although they’re probably less significant than often claimed. Folk wisdom suggests to avoid using MDMA more than once every three months. This rule seems to work great for users of MDMA, so it can’t hurt to follow it. Another reason to follow this rule is that according to a lot of people, repeated use of MDMA kills the “magic” of the experience, which you may never be able to get back. This is why many people like to spread out their uses.
Conclusion
To wrap up this section, I’ll say that I hope my support for the legalization of MDMA is understandable now. Wouldn’t it be wonderful if you could pick up a reasonable dose of real MDMA from a pharmacy or something, along with a list of the necessary precautions, without having to worry about all this drug testing and dosage nonsense? Too bad. This is impossible, because MDMA is illegal for recreational use and thus unregulated, and to add insult to injury, it’s also illegal for medical use. As a result we have people overdosing on unknown chemicals with the added risk of getting arrested and sent to jail. Ugh.
Risks and Non-Risks of Chronic Use of MDMA
From the results of Shulgin’s experimentation and the institution of MDMA-assisted psychotherapy, we know that with the right precautions (see previous section) it’s possible to be confident that you will never experience acute negative effects from using MDMA. Chronic effects are a different story, though, and I’ll cover the most common concerns here.
Addiction
MDMA is very enjoyable to use, so it’s reasonable to expect that it has some habit-forming potential. The results are surprising, at least to me. In a 2010 American national survey on drug use, 0.6% of MDMA-using Americans aged 12-24 reported ever becoming dependent on MDMA.23 In contrast, a review of surveys in English-speaking, developed countries found that two-thirds of respondents who had tried one cigarette became daily smokers24, and a 2017 survey of American adults found that 12.7% qualified for an Alcohol Use Disorder.25In fact, there is reason to believe that MDMA-assisted psychotherapy can resolve substance addiction. In one study, after one session of MDMA-assisted psychotherapy, 14 of 29 subjects reported a reduced desire for substances such as alcohol, cannabis, and caffeine, while 2 subjects reported an increased desire. This effect has pharmacological precedent. MDMA acts on serotonin receptors similarly to the classical psychedelics and prevents reuptake of catecholamine similarly to bupropion. Both of these other drugs are effective in the treatment of addiction.26
The addiction-treating potential of MDMA is currently being put into practice. An ongoing study published preliminary data in July of 2019 suggesting that MDMA-assisted psychotherapy is safe and effective in the treatment of Alcohol Use Disorder.27
Cognitive Deficits
Much has been said about the neurotoxicity of MDMA. Certain studies show all sorts of terrifying changes in the brain caused by MDMA use, but this doesn’t necessarily mean much in everyday experience, so I’ll focus on more straightforward and useful results: does MDMA cause cognitive deficits in practice? I’ll cover research on non-human animals first, then research on humans.There are many studies that demonstrate neurotoxic effects of MDMA, when administered repeatedly, in extremely large doses, to non-human animals. This tells us next to nothing about the neurotoxicity of MDMA when administered occasionally, in reasonable doses, to humans. I know this because if you make a rat binge drink for four days, it will develop brain damage,28 even though alcohol is well-tolerated in humans when used moderately. A systematic review published in July of 2019 found no evidence that doses of less than 3 mg/kg of MDMA, which are typical for recreational use, produced cognitive deficits in animals. Doses frequently ranging from 5 to 20 times greater than a common recreational dose also failed to produce cognitive deficits in the majority of experiments.29
There are also plenty of studies that detect impaired memory in regular human users of MDMA. A systematic review published in 2009 concludes that “A broad range of relatively low-quality literature suggests that recreational use of ecstasy is associated with significant deficits in neurocognitive function (particularly immediate and delayed verbal memory),” but that “deficits are likely to be relatively small.”30 Some studies fail to detect impaired memory in low to moderate users of MDMA, a population with an average of below 50 lifetime uses.31
A recent review carried out by the UK Advisory Council on the Misuse of Drugs suggests that the cognitive deficits detected by studies on MDMA users are “statistically significant, but not clinically significant.” Gabriel Rogers, the director of the review, claims that “[the memory and attention deficits] don’t seem to be very big and it’s not clear that they have much effect on day-to-day functioning.”32
Rogers also cautions that “It’s possible that ecstasy has horrific consequences later in life. Only time will tell.” Alexander Shulgin and his wife Ann consumed lots of MDMA (alongside about 230 other newly discovered chemicals) for large portions of their lives. Alexander Shulgin died at the age of 88 and was pretty mentally clear late in life, if rather eccentric, as evidenced by his later interviews. Ann Shulgin is still alive, aged 88, and still actively participates in the psychedelic community. Yes, this is a sample size of two, but the combination of sheer quantity of unusual drugs consumed and apparent absence of negative effects seems like it should tell us something. Somehow I’m not extremely concerned about the delayed cognitive consequences of MDMA use.
Depression
I’m feeling unmotivated about doing research for this part. I feel like it would turn out the same as the cognitive deficits section, especially since a bunch of studies I’ve seen suggest that the cognitive consequences of MDMA are more potent than the emotional ones. There are many (non-clinical) studies claiming depressed states in regular MDMA users, but there are bound to be lots of confounding factors. For example: your life probably isn’t going great if you want to use MDMA every two weeks or so, and oddly enough, the fact that your favorite hobby is illegal and highly stigmatized has the potential to make you feel depressed. The UK review I mentioned earlier claims that MDMA users are, on average, within the normal bounds on standard depression tests, although they do score worse than non-MDMA-users. Garcia Rogers says that “there is no indication that [MDMA users] are drifting out of normal functioning.” If you want to know whether MDMA will make you depressed, research it yourself and get back to me so I can expand on this. Thanks.Heart Problems
I looked for studies on MDMA cardiotoxicity. They were all very technical and didn’t tell me much about the practical consequences of MDMA use on my cardiovascular health. In this case I’m just going to copy and paste from the MAPS Investigator’s Brochure because I can’t think of much else to say on the subject:“Studies in Ecstasy users indicate that only people reporting average lifetime exposure of 900 tablets had cardiac abnormalities [287]. No abnormalities were found in people reporting lifetime exposure of approximately 200 tablets in the same study. Previous to this, echocardiographic readings in eight Ecstasy users also failed to find any cardiac abnormalities [52]. Valvular heart disease (VHD) only occurred after extremely heavy Ecstasy use; therefore, it is unlikely to be a risk within the research or therapeutic context where participants are screened for relevant preexisting conditions”
About the brochure: I’ve tried not to rely on it for this section of the post, but if you want more information about the health risks of MDMA, take a look at the MAPS Investigator’s Brochure. It’s incredibly thorough and covers pretty much anything you could think of.33
My main take-away from writing this section is that research can frame anything as dangerous if you do it right. Until recently, researchers seem to have been biased in favor of the conclusion that MDMA is dangerous. The truth is that, like basically everything, MDMA is benign in moderation and dangerous in excess, and moderate use of MDMA has some effects that potentially improve short-term and long-term emotional well-being
The Future of MDMA
Based on the contents of this post (which are probably biased and cherry-picked whether I realize this or not, so feel free to provide your own contradictory information), it’s clear to me that a country where MDMA is legal, well-known by the public, and widely available would be a better country than the one we currently have to deal with. The absence of widespread, accurate information about the risks and safe use of MDMA is a major detriment to public health. Despite widespread belief that MDMA is dangerous, large amounts of reckless people (usually young people who have not yet developed the ability to make good decisions, a population that I currently belong to) buy, sell, and use substances sold as MDMA or ecstasy anyway, and end up causing harm to themselves and others because they have no clue what they’re doing. Law enforcement contributes to this harm by sending users and vendors of MDMA to prison, in many cases ruining their lives. This situation is evidently absurd and it makes me angry. In fact, it’s making me more angry at the moment than probably anything else in existence.In the blighted world of American drug policy, one of the few beacons of light is an organization called the Multidisciplinary Association for Psychedelic Studies, or MAPS, founded in 1986, one year after the emergency scheduling of MDMA. As of August 2019, MAPS’ highest priority project is to sponsor Phase 3 studies of FDA research into MDMA for the treatment of PTSD. Their Phase 2 study in Boulder, CO produced amazing results: 12 months after treatment, 76% of participants no longer met criteria for PTSD. There were no serious adverse events and the treatment was well-tolerated.34 PTSD affects 7% of the U.S. population, and currently, the only FDA-approved medications for PTSD are SSRIs, which have extensive side effects and limited efficacy.35 MAPS plans to make MDMA into an FDA-approved prescription medicine for PTSD by 2021. Please, please, please consider donating to MAPS. You can do this here: https://store.maps.org/np/clients/maps/donation.jsp?campaign=11
MAPS is also currently conducting studies on MDMA for treatment of anxiety associated with life-threatening illness36 and social anxiety in autistic adults.37 The former currently stands at $218,000 raised out of the estimated cost of $627,000 and the latter currently stands at $28,000 raised out of $400,000. These studies have been ongoing since the early 2010s. After more than 30 years of neglect of this beautiful drug, research is still moving slowly. Why don’t people care? Hello?! Anyone? Antidepressants come with laundry lists of side-effects. Benzodiazepines cause one of the most deadly addictions known to humankind. Where is the support for MDMA, my dearest champion of love and conqueror of fear, to treat anxiety???
MAPS researchers claim that participants in studies of the effects of MDMA report “improved self‐knowledge, sleep regulation, accuracy in perceiving mental states of others, coping strategies, emotion regulation, and cognitive insights.”38 Could you look me in the eyes and tell me that MDMA cannot be described as penicillin for the soul? Could you look me in the eyes and tell me that MDMA cannot be useful at all for repairing and strengthening relationships, working through trauma, promoting compassion for yourself and others, and ultimately resolving a variety of emotional problems? Imagine if diplomats and world leaders took MDMA before meeting with each other, or everyone in a courtroom took MDMA before proceedings. What would happen? I don’t know, but it would be interesting for sure, and there’s at least a significant chance that it would be productive for the future of humanity.
I’ll end with the words of Dr. Ben Sessa, the director of a study I mentioned earlier on MDMA for the treatment of Alcohol Use Disorders. In an interview about the study, Dr. Sessa was asked, “Aren’t there still grounds for concern over the potential dangers of prescribing a drug that has been so under-studied in the past?” Dr. Sessa replied, “Yes, that’s true. I ought not to promote all those toxic drugs such as Quetiapine, Olanzeopine, Seroxat, Ritalin, Lithium, Diazepam, Prozac, Penicillin, Carbamazepine and cancer chemotherapy drugs. They are indeed all very toxic. Truth is, the psychedelic drugs are considerably less toxic than pretty much any other drug I use with my patients on a daily basis. The reason why I am interested in psychedelic medicine is because I don’t like those toxic drugs listed above. Psychedelic therapy offers patients the best opportunity we have to get them off all that stuff and live a drug-free life.”39 To add to Dr. Sessa’s wisdom, I don’t think a drug-free life is necessarily healthy, desirable, or much fun at all, but maybe that’s just me.
Bibliography
1 https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHDetailedTabs2017/NSDUHDetailedTabs2017.pdf↩
2 https://journals.sagepub.com/doi/pdf/10.1177/0269881107084738↩
3 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4678620/↩
4 https://www.jneurosci.org/content/39/2/307↩
5 https://s3-us-west-1.amazonaws.com/mapscontent/pdfs/MDMA-Annual-Report_FINAL_30DEC2016.pdf↩
6 Bernschneider-Reif S, Oxler F, Freudenmann RW (November 2006). "The origin of MDMA ("ecstasy")--separating the facts from the myth". Die Pharmazie. 61 (11): 966–72. doi:10.5555/phmz.61.11.966 (inactive 29 June 2019). PMID 17152992.↩
7 https://maps.org/news/media/5993-playboy-ecstasy-was-legal-in-1984,-and-it-was-glorious↩
8 Holland J (2001). "The History of MDMA". In Holland J (ed.). Ecstasy: the complete guide; a comprehensive look at the risks and benefits of MDMA. Rochester, VT: Park Street Press. ISBN 978-0-89281-857-0.↩
9 https://www.ecstasydata.org/stats.php?style=percent&datetype=testingdate&source=&sold_as_ecstasy=both↩
10 https://harmreduction.org/issues/fentanyl/↩
11 https://erowid.org/chemicals/mdma/mdma_dose.shtml↩
12 https://www.ncbi.nlm.nih.gov/pubmed/19195429↩
13 https://www.gov.uk/government/statistics/drug-misuse-findings-from-the-2017-to-2018-csew↩
14 https://dancesafe.org/heatstroke/↩
15 https://dancesafe.org/mdma-related-deaths-stop-calling-them-overdoses/↩
16 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2957712/pdf/IJPsy-42-195.pdf↩
17 https://dancesafe.org/drug-information/mdma-contraindications/↩
18 https://dancesafe.org/mdma-related-deaths-stop-calling-them-overdoses/↩
19 https://dancesafe.org/drug-information/mdma-contraindications/↩
20 https://medlineplus.gov/ency/article/001315.htm↩
21 https://www.researchgate.net/profile/Nele_Samyn/publication/8779340_Dissociable_Effects_of_a_Single_Dose_of_Ecstasy_MDMA_on_Psychomotor_Skills_and_Attentional_Performance/links/548ec9b30cf2d1800d846668.pdf↩
22 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395348/↩
23 Substance Abuse and Mental Health Services Administration. Results from the 2010 National Survey on Drug Use and Health Summary of National Findings. Rockville, MD: Substance Abuse and Mental Health Services Administration 2011 Contract No.: 11-4658 ↩
24 https://www.ncbi.nlm.nih.gov/pubmed/29126298↩
25 https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2647079↩
26 http://www.maps.org/research-archive/mdma/Jerome_CDAR_30Apr13.pdf↩
27 https://casereports.bmj.com/content/12/7/e230109 ↩
28 https://www.ncbi.nlm.nih.gov/m/pubmed/12878913/↩
29 http://pharmrev.aspetjournals.org/content/71/3/413↩
30 https://www.ncbi.nlm.nih.gov/pubmed/19195429↩
31 http://www.maps.org/research-archive/mdma/Jerome_CDAR_30Apr13.pdf↩
32 https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/119088/mdma-report.pdf↩
33 https://mapscontent.s3-us-west-1.amazonaws.com/research-archive/mdma/MDMA-Investigator-Brochure-IB-11thEdition-MAPS-2019-07-10.pdf↩
34 https://journals.sagepub.com/doi/full/10.1177/0269881118806297↩
35 https://maps.org/news/multimedia-library/2890-new-treatments-to-combat-post-traumatic-stress-disorder↩
36 https://maps.org/mdma-assisted-psychotherapy-for-anxiety-associated-with-life-threatening-illness↩
37 https://maps.org/research/mdma/anxiety/autism↩
38 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5260336/↩
39 https://filtermag.org/inside-an-innovative-study-of-mdma-therapy-for-alcohol-use-disorder/↩